The VERSE Equity Toolkit was officially launched on 25th May 2022.
Objective: To provide countries with robust evidence on the economic and equity implications of their immunization financing and delivery strategies.
Primary components:
Vaccine equity assessment methodology & toolkit
Country case studies: stimulate and tracking the use of equity metric in policymaking and program evaluation
Vaccine-related outcomes (metric):
Programmatic equity: vaccine coverage (% coverage)
Economic equity: VPD-related costs and benefits (US$ or local currency)
Health outcomes equity: DALY averted due to vaccine coverage (DALY)
Toolkit properties:
Multi-dimensional composite metric: SES, settings, region, sex, maternal education, health insurance
Decomposable: We can isolate the dimensions in the composite metric
Flexible data input: public datasets (DHS, LSMS), government data (HMIS, DHIS2), private/study data (e.g., MATCHES)

To identify what issues impair vaccine coverage, researchers traditionally look for an association with just one variable—wealth, for example—instead of examining the host of factors in play. Typical equity metrics may not appropriately account for the compounding effect of geographic and sociodemographic factors on immunization outcomes, such as, in the case of pediatric immunization, where a household is located, the sex of a child being vaccinated, and maternal education level.
Additionally, when considering issues of equity rather than equality using global health data, it is necessary to account for factors that influence need and eligibility instead of looking at crude disparities. When examining equity in routine pediatric vaccine coverage, need can be simplified to whether a child is old enough to receive a vaccine, while for adult vaccines, need may be multifaceted and include age, risk, and vulnerability criteria.
The Vaccine Economics Research for Sustainability and Equity (VERSE) project developed a toolkit that uses novel methodologies to rank a country’s population by level of composite disadvantage which is composed of known factors that fairly and unfairly influence access to and uptake of vaccines.
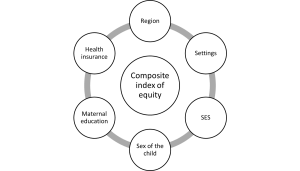
For routine pediatric vaccines, fair factors include whether the child is too young to receive a vaccine based on the national immunization schedule. Unfair factors include the household’s region, setting (urban/rural), and socioeconomic status (SES), as well as the sex of the child, level of maternal education, and whether the household is covered by any health insurance (Figure 1).
The VERSE Equity Toolkit can utilize data from any recent Demographics and Health Surveys (DHS) to generate estimates for vaccine coverage and several indicators for vaccine equity. The vaccine equity measures can be used to compare countries, regions, or subnational localities, at one point in time or across time, and measure and track progress in reducing gaps in coverage between the most vulnerable and most advantaged. The toolkit also runs decomposition analyses to reveal the share that each factor contributes to the measured inequity in vaccine coverage.
The full methodology is detailed in “A standardized approach for measuring multivariate equity in vaccination coverage, cost-of-illness, and health outcomes: Evidence from the Vaccine Economics Research for Sustainability & Equity (VERSE) project” published in Social Science & Medicine on April 16, 2022.
This study demonstrates the use of the VERSE Equity Tool using the 2015-2016 India DHS.
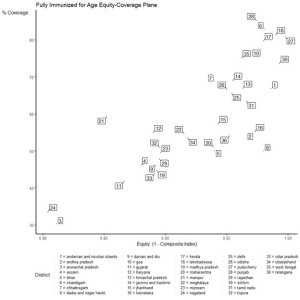
Using the VERSE Equity Tool, it was found that the proportion of children fully immunized for their age in each state was negatively correlated with the level of (composite) equity. Half of India’s states achieved between 45% and 60% coverage, equity levels varying between 0.87 and 0.98 (Figure 2). Arunachal Pradesh (#3) and Nagaland (#24) have the lowest levels of both coverage and equity.
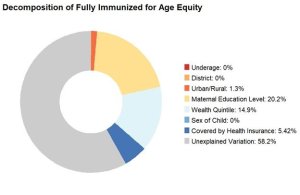
Maternal education level appears to be the largest contributor (20.2%) to the variation in fully-immunized status (Figure 3), followed by socioeconomic status (14.9%) and then, household health insurance status (5.4%). Children whose mothers have achieved a lower level of education are more likely to drop out of the immunization schedule by the age of two.
The International Vaccine Access Center (IVAC) at the Johns Hopkins Bloomberg School of Public Health spearheaded the development of the VERSE Equity Tool with funding from the Bill & Melinda Gates Foundation.
Makerere University School of Public Health, the Postgraduate Institute of Medical Education & Research, and the Maternal and Child Health Center in India are investigating the effect of maternal educational achievement on the use of antenatal and neonatal care and vaccination services in Uganda and India. Low achievement in maternal education was significantly associated with children dropping out of the immunization schedule and those never receiving any vaccine (zero-dose status).
Peking University estimated geographic, sociodemographic, and socioeconomic inequalities in coverage for vaccines included in China’s National Immunization Program (NIP) and non-NIP vaccines. The team’s report was tailored to help regional and national policymakers make a stronger case for investment in vulnerable communities.
The International Centre for Diarrhoeal Disease Research, Bangladesh is applying the VERSE Equity Tool on primary household and patient-caregiver data to assess inequity in vaccine coverage and vaccine-preventable disease outcomes, such as the cost of illness. The data were collected between September 2021 and March 2022 in collaboration with IVAC.
The University of Gondar School of Pharmacy, in collaboration with the Ministry of Health of Ethiopia, is assessing the factors that contribute to the high prevalence of zero-dose status among children in Ethiopia.
The VERSE team consists of Bryan Patenaude, Gatien de Broucker, Joshua Mak, Salin Sriudomporn, and Deborah Odihi.
To get involved in the VERSE project or discuss adaptations of the Equity Tool for different datasets and analyses, please contact Bryan Patenaude bpatenaude@jhu.edu
Image credit: UX Indonesia for unsplash.com
Any organization or individual working in the field of immunization economics can submit findings, opportunities, calls to action, or other relevant work below to be shared with our community.