By Laura Boonstoppel and Flavia Moi, ThinkWell
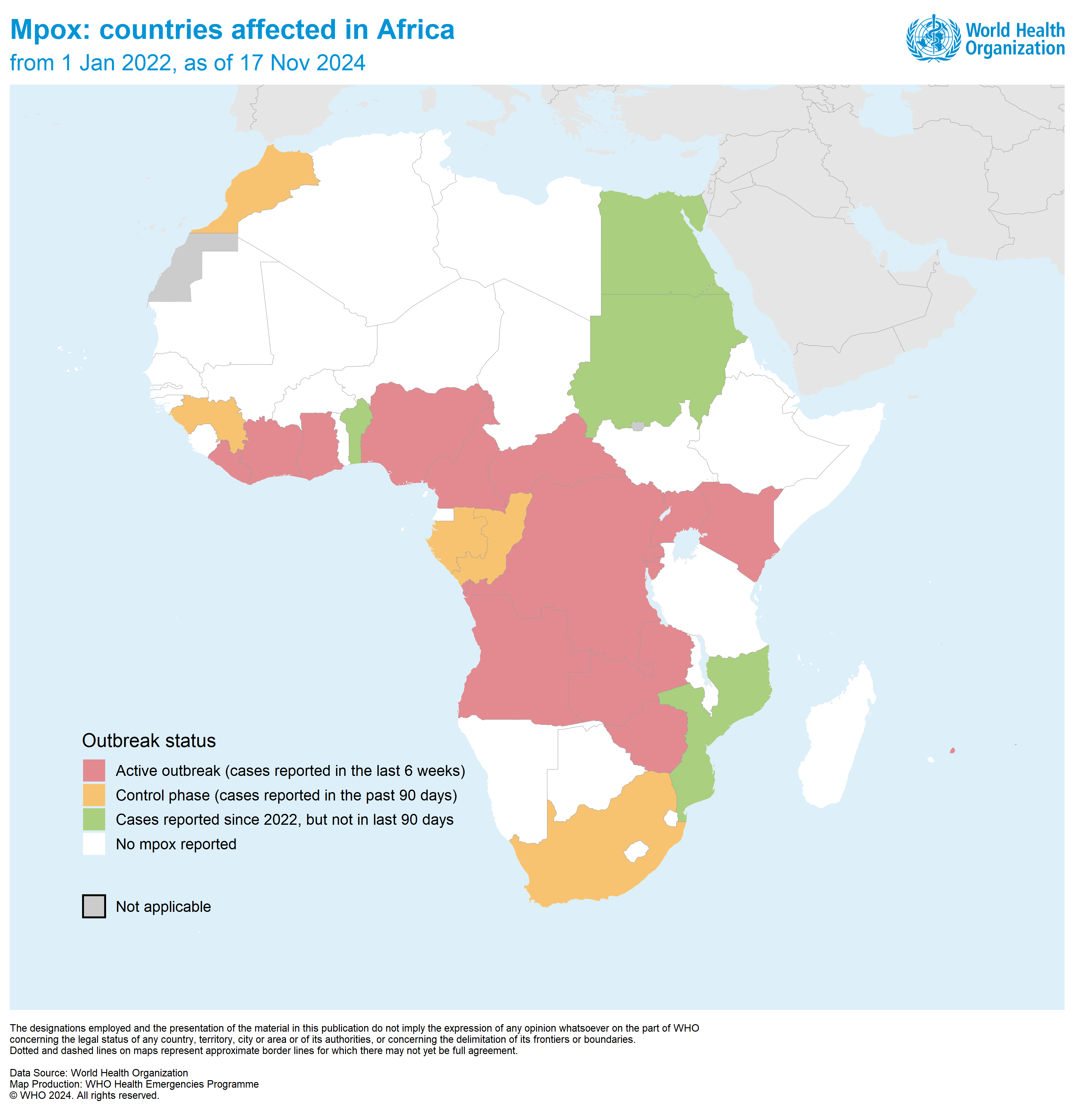
Africa is currently battling the worst mpox outbreak ever, with 24 countries having reported over 48,000 cases, many more than during any previous outbreak. The Democratic Republic of the Congo (DRC) is by far the hardest hit, with more than 1,100 deaths recorded this year. Building on learnings from the COVID-19 experience, global partners mobilized at record speed to get mpox vaccines into the DRC and other endemic countries, a tremendous success.

© World Health Organization / Guerchom Ndebo / 2024
However, mpox vaccines are new, and the cost of delivering them is highly uncertain. Delivering mpox vaccines may be much more expensive than other vaccines that African countries have delivered in the past. With the Access and Allocation Mechanism for mpox (AAM) having recently allocated 899,000 doses to nine countries in Sub-Saharan Africa, and many more doses promised by the end of 2024, it is crucial to understand the cost of delivering mpox vaccines.
In this blog post we look at the case of the DRC, the epicenter of the mpox outbreak, and examine what we know about vaccine delivery costs to answer the question: what does it cost to deliver mpox vaccines?
A rapid increase in mpox cases led the Africa CDC to declare mpox a public health emergency of continental security on August 13th 2024. The day after, the WHO declared it a public health emergency of international concern. Twenty countries in Africa have reported cases just this year, with the overwhelming majority being in the DRC (93%).
Mpox is not a new disease, and was first reported in the DRC in 1970. Mpox steadily emerged in central, east and west Africa following the eradication of smallpox in 1980, and with that, the end of worldwide smallpox vaccination. Since then, there have been sporadic reports of mpox cases in African countries, and in 2022, an outbreak appeared suddenly and rapidly spread globally. The outbreak was quickly contained thanks to behavioral change interventions and prompt vaccination of at-risk populations, mainly men who have sex with men (MSM).
What is different this time? The current outbreak is fueled by a new offshoot called clade Ib, which has been suspected to be more severe. In addition, it has not been contained to MSM and sex workers but also spread through the general population. This time, it is also affecting children who are four times more likely to die from the disease.
In August 2024, WHO recommended mpox vaccination for all communities at high risk of exposure to the disease, and by September, a first mpox vaccine (MVA-BN) received WHO prequalification. The international community acted quickly to get mpox vaccines to the DRC—initially through donations from the United States, the European Union, and Bavarian Nordic. By October 5th, 265,000 doses had arrived in the country, and the DRC launched its first mpox vaccination campaign in the hardest-hit provinces. Since then, over 51,000 people have been vaccinated across 6 provinces. Mid-November, the DRC received an additional 100,000 doses, to support the delivery of second doses to those who were vaccinated during the October campaign, as well as for vaccinating in additional hotspots, including in Kinshasa.
Vaccination has also begun on a limited scale in Rwanda, and Nigeria, and five other countries will also receive mpox vaccines soon: Central African Republic, Côte d’Ivoire, Kenya, Liberia, South Africa and Uganda. In total, the Access and Allocation Mechanism for mpox promises to have over 5.85 million vaccine doses available by the end of the year.

Mpox vaccines are relatively new, and there are a number of reasons why the cost of getting the vaccines from their arrival in a country down into the arms of those who are most at risk might be higher than the cost of delivering routine vaccines, or even compared with other outbreak responses.
All prequalified mpox vaccines come in a single-dose presentation which takes up a lot of space in the cold chain. A dose of an mpox vaccine takes up to about 10 times as much space as a measles vaccine, which makes it expensive to transport and store. As is the case in many of the mpox-endemic countries, the DRC lacks sufficient cold chain equipment at lower levels of the health system. This means that vaccination sites cannot store enough doses, and many more trips are needed to supply them with mpox vaccines, which pushes up transport costs.
The supply of mpox vaccines is severely constrained, and lessons learned from the COVID-19 vaccine rollout show that this can increase delivery costs considerably. Just like during the early days of the COVID-19 vaccine response, mpox vaccines are shipped across the DRC in small batches. Although MVA-BN is much more stable than COVID-19 and Ebola vaccines, and can be kept at refrigerated temperature for double the time, mpox vaccines still need to be distributed as soon as they are available to ensure a rapid vaccination response.
So far, the first vaccination campaign in the DRC reached 51,000 people across 6 provinces. Reaching so few people among a total population of over 27 million and across a combined surface larger than France is likely to lead to high transport costs. The situation is likely similar in Nigeria, which is currently delivering just 10,000 doses across 7 states.
The overall low delivery volume means that one-off costs like training, and overhead costs like technical assistance also weigh more on the cost of each dose delivered. During Ebola vaccination efforts, international technical assistance was a key cost driver, which is likely to be the case for the mpox response as well.
Until today, only the MVA-BN vaccine has been used in the mpox response, but donor pledges include two others: ACAM2000 and Japan’s LC-16 vaccine, and the latter just received WHO approval this week. While this will help alleviate supply constraints, the COVID-19 vaccine roll out has shown that use of multiple vaccine products can increase delivery cost, as health workers need to be trained on each new vaccine when it becomes available.
The two additional mpox vaccines both require the use of a bifurcated needle, a tool specific to smallpox vaccines that most vaccinators today are not familiar with, which will require additional investments in training for health workers. The various mpox vaccines are also authorized for a slightly different target population, and health workers will need to be trained on managing the differences.
The MOH aims to vaccinate 2.5 million people with 3.5 million doses. Given the limited supply, selected populations were prioritized for the October campaign: frontline workers, sex workers, transgender people, MSMs, eco guards, mpox contact cases, and other vulnerable populations including those with compromised immune systems. Identifying and reaching specific priority groups is not straightforward and doing this effectively can be costly. The first phase of the campaign has shown that estimating the number of contact cases upfront is challenging, and these were considerably underestimated.
Additionally, prioritization strategies need to be adequately communicated, as learnings from Ebola show that uncertainty around who is eligible to get the vaccine can fuel misinformation. For instance, during the DRC’s first vaccination campaign, there were concerns in the community around why children were not prioritized for vaccination, as mpox is more dangerous for them. In fact, the DRC’s mpox vaccination strategy aimed to prioritize children, but at the time, the MVA-BN vaccine was only licensed for use in adults. Shortly after, the WHO extended it to 12-17 year olds, and the newly approved LC-16 vaccine is licensed for use in this age cohort as well, so communication strategies will need to adapt to these changes.
As more vaccines become available, and eligibility for mpox vaccines evolves, communication around eligibility and prioritization needs to be carefully managed. Each new target group needs to be informed and mobilized, which increases the costs of social mobilization.
The DRC has a documented history of vaccine hesitancy, and traditionally requires extensive community engagement to ensure sustained demand. Studies have shown vaccine acceptance to be even lower for outbreak responses than for routine vaccination. A high level of vaccine hesitancy, including among health workers, was a major challenge during the COVID-19 vaccine rollout, when it significantly decreased vaccine uptake. The low uptake ultimately pushed up the cost per dose delivered.
During the first mpox vaccination campaign in the DRC, vaccine hesitancy was not reported to be an issue, though this may change in the next phase of the campaign among communities that have had less exposure to deaths and severe cases. Vaccine acceptance for mpox is currently higher than it was for COVID-19 vaccines, but is still only about 61% among health workers. Consistent investments to sustain demand among the growing target population will be needed. The Ebola experience in the DRC teaches us that earning community trust during an outbreak vaccination response can be challenging and requires investments in effective, targeted social mobilization strategies.

The provinces of North Kivu and South Kivu, which are the epicenter of the current outbreak in the DRC, have been home to a series of protracted armed conflicts which have caused the displacement of over 2.7 million people in 2024 alone. Conflict has strained the health system infrastructure needed to distribute vaccines, and delivering vaccines in this context likely comes at a much higher cost. Mpox vaccines will need to reach the most vulnerable communities, including in refugee and internally displaced persons camps, which requires additional support from partners and can be costly.
In addition, the presence of armed groups may limit the government’s ability to distribute mpox vaccines everywhere. So far, the government has been solely responsible for delivering mpox vaccines, but in future phases of the campaign, reaching areas controlled by armed groups may require contracting non-governmental implementing partners, which could drive up the costs considerably.
While delivery costs for mpox vaccines are unknown, existing evidence can help us understand how the context of this outbreak and the way its vaccination response is implemented may affect delivery costs. While the cost of delivering regular childhood vaccines in a low- or middle-income country is about $1.34 per dose, evidence from COVID-19 vaccine delivery and Ebola vaccination shows that the unit cost of delivery can be much higher for a new vaccine that is introduced in the context of an epidemic, especially in conflict-affected areas.
During the early days of the COVID-19 vaccine roll-out, the additional financial cost of delivering a single dose in the DRC was as high as $3.12, and even higher in rural areas ($3.27), due to the piece-meal supply, vaccine hesitancy, and complexities of identifying and reaching the narrow priority target population.
Mpox delivery costs are likely even higher. COVID-19 vaccines come in a more space-efficient 10-dose presentation, and the COVID-19 vaccine rollout was plagued by funding shortages and delays, while the mpox vaccination campaign has thus far received adequate support.
Especially in conflict-affected areas, the cost of mpox vaccine delivery is likely much more significant. Delivering Ebola vaccines in North Kivu, Ituri, and South Kivu during the 10th outbreak costed as much as $22 per dose* which demonstrates the increased cost of delivering vaccines in a conflict-affected settings.
Outbreak responses often use campaigns to quickly and cost-efficiently deliver vaccines in large volumes to a targeted group. So far, supply constraints have prevented the delivery of mpox vaccines at scale. As we have seen during the COVID-19 vaccine roll-out, when supply constraints ease and the target population expands, larger vaccine delivery volumes allow for increased efficiencies in vaccine distribution and delivery strategies that can dramatically bring down the delivery cost per person reached.
Targeting highly concentrated populations in urban settings, such as the DRC’s effort to vaccinate prisoners in Kinshasa, will also allow the program to more efficiently reach a larger number of people per day, reducing the cost per dose delivered.
Donors and manufacturers can support this by ensuring a rapid ramp up of supply and coordinated shipments to optimize the delivery of mpox vaccines.
So far, vaccine hesitancy for mpox vaccines has been relatively limited in the DRC, but this is likely to change when the vaccine is rolled out to a larger population that is more distant from the impact of the disease. During the first year of the DRC’s COVID-19 vaccination program, due to a lack of demand and high vaccine hesitancy, vaccines expired or were redeployed to other countries, a huge cost to the program that further damaged the public’s trust in the vaccine.
To prevent vaccine hesitancy, the country can leverage learnings from Ebola, which show that community trust in vaccination can be improved by making information available in local languages, and adequately engaging local influencers. Building and sustaining trust in a new vaccine can be costly, but the consequences of low vaccine uptake and a continued mpox outbreak will be much costlier.
Donors and partners can build on learnings from COVID-19, where social mobilization was recognized as a key need yet highly underfunded, and provide support to the DRC to ensure the development and implementation of a comprehensive social mobilization strategy.
Measles vaccination coverage is extremely low in the DRC, one of the lowest in the world, especially in the most vulnerable areas affected by mpox. Measles cases have been rising in South Kivu and North Kivu since this year’s mpox outbreak, leading to several cases of co-infections of mpox and measles. This comorbidity may partly explain the increase in deaths among children reported during this outbreak, and underlines the importance of sustaining and boosting vaccination coverage for measles and other vaccine-preventable disease amidst this epidemic.
The COVID-19 experience has shown that an epidemic response can disrupt the delivery of essential health services, including immunization, and cause potentially long-lasting consequences on their coverage, sometimes leading to outbreaks of even deadlier diseases.
The DRC and other mpox endemic countries can protect coverage for essential health services while reducing the cost of the mpox vaccination program by integrating delivery with other health services. So far, mpox vaccine delivery has been a standalone operation, despite identified opportunities to co-deliver, for example, condoms to sex workers. The inclusion of children in the DRC’s next vaccination campaign will unlock more opportunities for integrated delivery, including with routine immunization. This will bring the cost of mpox vaccine delivery down while also reaching vulnerable communities with other life-saving vaccines.
Donors and partners can support integration by improving coordination among different vertical programs, synchronizing shipments of commodities, and aligning on the planned timing of grants, supplies, interventions, and reporting.
Currently, delivery costs for mpox vaccines are high. In a context like that of the DRC and similar countries, which face extreme resource scarcity and many competing health priorities, delivery costs must be brought down. Countries, donors, and partners can help achieve this by ensuring a rapid ramp up of mpox vaccine supplies, investing in social mobilization to sustain demand for the vaccine, coordinating shipments, and facilitating integrated delivery.
Finally, while mpox delivery costs are high, they pale in comparison to procurement costs for the vaccine. Mpox vaccines currently cost about $65 per dose, which is more than a hundred times as much as UNICEF’s most expensive measles vaccine. Given the tight funding landscape and the many priorities that the global health community faces today, donors must use all the market shaping tools at their disposal to bring the price of mpox vaccines down, and ensure adequate financing for all health programs.
*Deducting an assumed vaccine price of 98.6 USD per dose as per UNICEF Supply Division data
Acknowledgements: We would like to thank Dr Nanou Yanga Mukadi (Ministry of Health, DRC), and Cyril Nogier (Gavi, the Vaccine Alliance) for their valuable contributions to contents of this blog.
This blog was written by Flavia Moi (Senior Technical Advisor, fmoi@thinkwell.global) and Laura Boonstoppel (Program Director, lboonstoppel@thinkwell.global) at ThinkWell.
